15 year old with anemia under evaluation
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Unit II admission on 02/03/2021
DR. JAYANTH ( INTERN)
DR. AMULYA ( INTERN)
DR. SURYA PRADEEP ( INTERN)
DR. ASHA KIRAN ( INTERN)
DR. YAMINI ( INTERN)
DR. VAMSHI ( INTERN)
DR. ISMAIL (INTERN)
DR. PRADEEP ( PG 1st YEAR)
DR. DIVYA( PG 2nd YEAR)
DR. SUFIYA ( PG 3rd YEAR)
DR. SATISH ( PG 3rd YEAR)
Faculty : DR. VIJAYALAXMI
Here is a case i have seen:
A 14 year old boy studying 8th standard presented with chief complaints of pain abdomen since 1 month loss of appetite since 1 month, poor stream of urine since 10 days and fever since 6 days.
Patient was apparently alright 1 month back then he had abdominal pain which was insidious in onset associated with 2 episodes of vomitings and loose stools for 2 days, subsided after taking medication abdominal pain is associated with loss of appetite
From 10 days patient is having poor stream of urine associated with dribbling of urine after micturition not associated with any burning micturition and from 6 days patient is having low grade fever continuous relieves on taking medication from 2 days patient is having evening rise of temperature associated with chills and rigors relieves on taking medication, not associated with cough, headache, tinnitus, burning micturition, ear discharge, ear pain.
No past history of type 1 DM, HTN, asthma, tuberculosis.
Regular bowel movements,
No known allergies
On examination:
There are signs of pallor.

No signs of icterus, cyanosis, clubbing, lymphadenopathy, pedal edema

Vitals:
Temperature: 98.2F
PR: 92/min
BP: 100/60 mmhg
RR: 22/min
SpO2: 98% on RA
CVS- S1 S2 heard
RS- bilateral air entry present
P/A- soft nontender
CNS- higher mental functions intact
No focal deficits
Provisional diagnosis:
? Anemia under evaluation
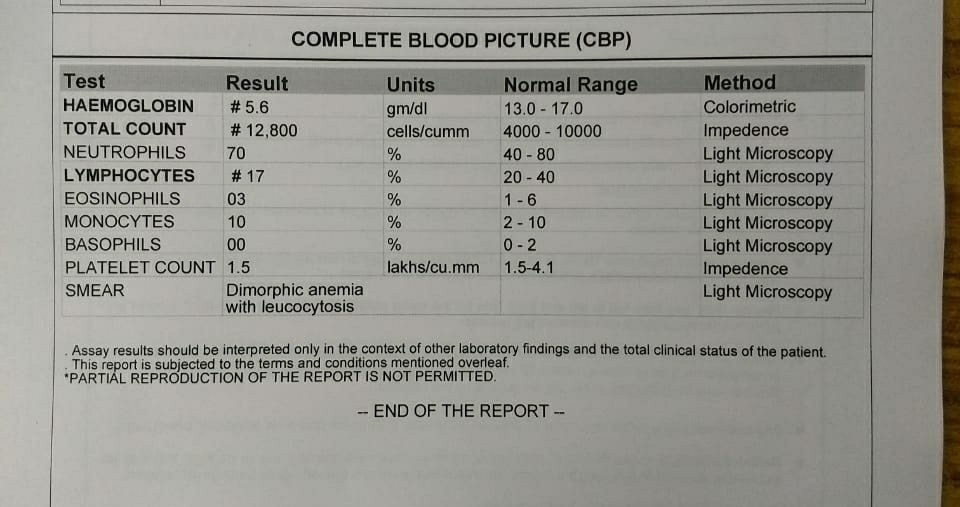
Investigations:



Treatment: on day of admission (02/03/2021)
Tab pan 40mg/ OD
Tab. PCM 500mg/ TID
Temp charting 4th hourly
GRBS charting 8th hourly
TREATMENT on day 1 (03/03/2021)
S-
Increased fever spikes yesterday night.
Loss of apetite.
Dark coloured stools passed.
Pain abdomen on/off.
O-.
Patient is c/c
SBP-120mmhg
PR-120bpm
Pallor present.
CVS-S1S2 heard, apical impulse 1cm medial to MCL in 5th ICS.
RS-BAE present.
CNS- No FND
PA-Soft and non tender, liver and spleen not palpable.
No palpable lymph nodes.
A-
ANEMIA UNDER EVALUATION.
P-
1.Tab PAN 40mg/ OD
2.Tab. PCM 500mg/ TID
3.T. ALBENDAZOLE 400mg PO STAT.
4.Temp charting 4th hourly
5. Teppid sponging SOS.
6. Inj. ARTESUNATE 120mg 0,12,24hrs.
7. BP, PR, RR monitoring.
8. Inj. IRON SUCROSE 1amp in 100ml NS over 30mins.

Sr. LDH- 154
PS- Microcytic hyprochromic anemia
TREATMENT on day 2 (04/03/2021)
S-
Stomach pain decreased.
Appetite improved.
No urinary symptoms.
No fever spikes.
O-
Patient is c/c.
Temp-98F
BP-110/40mmhg
PR-118/min
CVS-s1s2 present
RS-BAE+
CNS-No FND
PA-Soft, NT
A-
IRON DEFICIENCY ANEMIA
P-
1.Tab PAN 40mg/ OD
2.Tab. PCM 500mg/ TID
3.Temp charting 2nd hourly
4. Teppid sponging SOS.
5. Inj. ARTESUNATE 120mg 0,12,24hrs.
6. BP, PR, RR monitoring.
7. Inj. IRON SUCROSE 1amp in 100ml NS over 30mins.





TREATMENT on day 3 (05/03/2021)
S-
No new complaints
Fever spikes +
O-
pt is c/c
Bp- 110/50mmhg
PR- 118/min
CVS- S1S2 heard
RS- B/LAE+
CNS- no focal deficits
P/A- soft non tender
A-
IRON DEFICIENCY ANEMIA
P-
Rx;
1.Tab. Pan 40mg/PO/OD
2.Tab. PCM 500mg/ PO/ TID
3.Inj. IRON SUCROSE 1 amp in 100 ml NS over 30min / BD
4.Temp charting 2nd hourly
5.BP, PR, SpO2, RR monitoring
6.Tepid sponging
7.Thrombophobe ointment for L/A
8. T. NORFLOXACIN BD started night after getting c/s reports.


TREATMENT on day 4 (06/03/2021)
S-
No new complaints
Fever spikes +
O-
pt is c/c.
Bp- 110/50mmhg
PR- 106/min
CVS- S1S2 heard
RS- B/LAE+
CNS- no focal deficits
P/A- soft non tender
A-
IRON DEFICIENCY ANEMIA
P-
Rx;
1.Tab. Pan 40mg/PO/OD
2.Tab. PCM 500mg/ PO/ TID
3.Inj. IRON SUCROSE 1 amp in 100 ml NS over 30min / BD
4.Temp charting 2nd hourly
5.BP, PR, SpO2, RR monitoring
6.Tepid sponging
7.Thrombophobe ointment for L/A
8. T. NORFLOXACIN 400mg PO BD.




Comments
Post a Comment